
Introduction
DHT is the final amplifier of the androgenic signal, but it requires a precursor. That precursor is testosterone, and testosterone production depends on Leydig cells in the testes responding appropriately to stimulation. When Leydig cells work well, testosterone flows, and DHT follows.
Human Chorionic Gonadotropin (hCG) is an FDA-approved hormone that mimics Luteinizing Hormone (LH), directly stimulating Leydig cells to produce testosterone. Unlike upstream interventions that work through the hypothalamus and pituitary, hCG goes straight to the source -- activating testicular testosterone production regardless of what is happening higher in the cascade.
For DHT optimization, this direct approach has clear advantages. By ensuring robust testosterone production, hCG provides the substrate pool that 5-alpha reductase needs to produce DHT. In this article, you will learn how hCG supports DHT through testosterone production, why this matters for androgenic function, and how FixMyT helps you understand your individual androgen dynamics.
Understanding DHT: The Amplification of Your Metabolism
In the FixMyT metabolic tree, DHT occupies Level 4: Androgen Expression with the subtitle "Amplification." This is not metaphorical -- DHT literally amplifies the testosterone signal through several mechanisms:
- Superior receptor binding: 5x higher affinity for androgen receptors than testosterone
- No estrogen conversion: Cannot be aromatized, maintaining pure androgenic signal
- Sexual function driver: Essential for libido, erection quality, and sexual response
- Neurological effects: Drives confidence, assertiveness, and motivation
- Tissue-specific actions: Critical in prostate, skin, hair follicles, and brain
When DHT is insufficient, symptoms often appear as low libido despite adequate testosterone levels, reduced erectile quality, diminished confidence, and a sense of "something missing" despite good lab numbers. This is the DHT gap -- where testosterone looks fine but the androgenic signal is not being properly amplified.
The solution is not always at the DHT level. Often, the substrate is the problem. Without adequate testosterone production, 5-alpha reductase has nothing to work with. hCG addresses this at the testicular level.
What Is hCG?
Human Chorionic Gonadotropin is a naturally occurring hormone produced during pregnancy. In males, it mimics LH and directly stimulates Leydig cells to produce testosterone. This makes it invaluable for maintaining testicular function and testosterone production.
Key characteristics of hCG:
- Classification: Gonadotropin hormone
- FDA status: Approved for fertility and hormonal conditions
- Mechanism: LH receptor agonist on Leydig cells
- Administration: Subcutaneous or intramuscular (250-500 IU, 2-3x weekly typical)
- Half-life: 24-36 hours
- Unique feature: Direct testicular stimulation, bypassing pituitary
hCG has been used in medicine for decades, giving it one of the longest safety records of any hormonal intervention. It is particularly valuable for men on TRT who want to maintain testicular function and intratesticular testosterone levels.
For the complete technical profile, see the full hCG profile on PepGuide.
How hCG Supports DHT Function
The relationship between hCG and DHT operates through testosterone as an intermediate. The pathway is direct and clinically well-established:
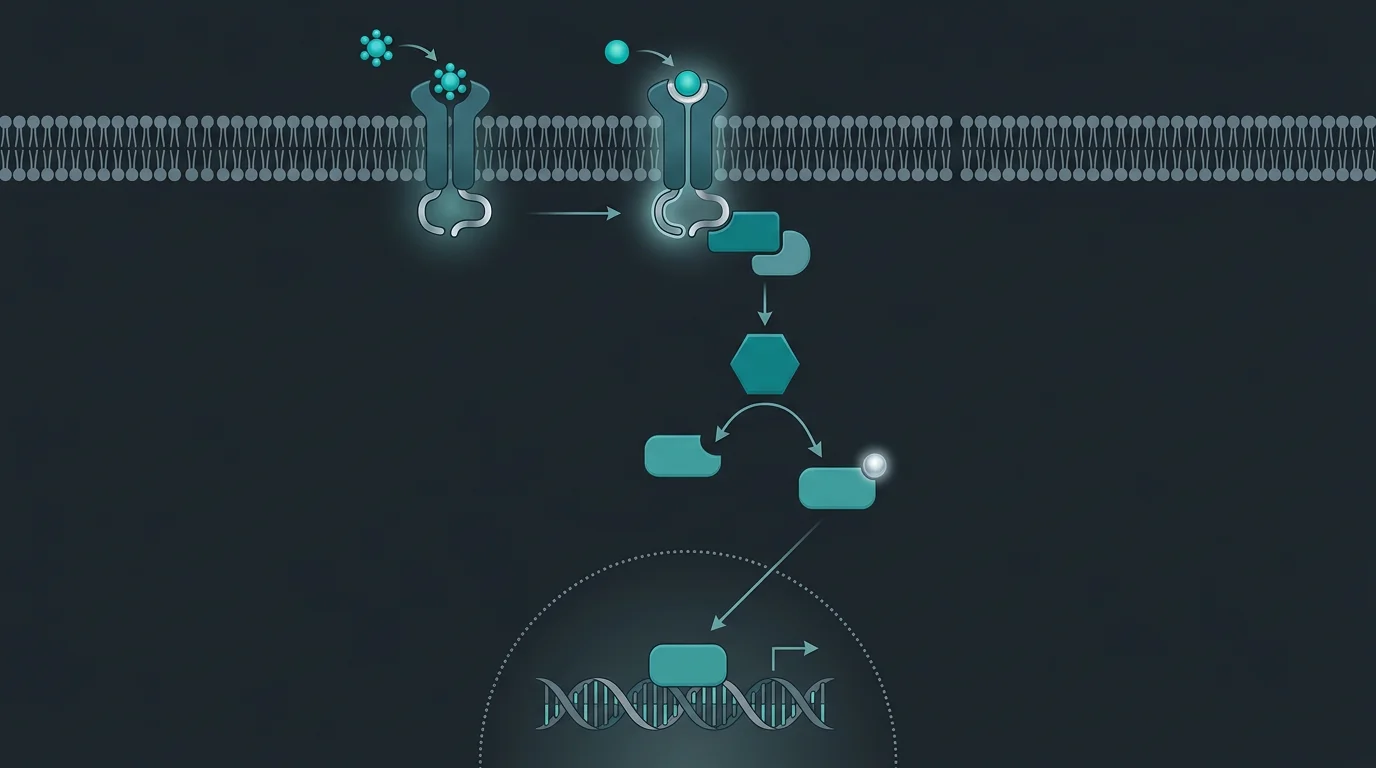
1. Direct Leydig Cell Stimulation
hCG binds to the same receptors as LH on Leydig cells:
- Activates cAMP signaling cascade
- Stimulates cholesterol transport into mitochondria
- Activates StAR protein (rate-limiting step in steroidogenesis)
- Triggers full testosterone synthesis pathway
This happens regardless of what is occurring upstream. Even if the hypothalamus and pituitary are suppressed (as in TRT), hCG can still stimulate testosterone production.
2. Intratesticular Testosterone Maintenance
Intratesticular testosterone (ITT) concentrations are crucial:
- ITT is 40-100x higher than serum testosterone
- This high local concentration supports Sertoli cell function
- Also supports local 5-AR activity
- hCG maintains ITT even when exogenous testosterone suppresses LH
High intratesticular testosterone creates the optimal environment for 5-alpha reductase to produce DHT locally and for overall androgenic function.
3. Substrate Provision for 5-AR
With adequate testosterone production ensured:
- 5-alpha reductase Type 1 and Type 2 have substrate to work with
- DHT conversion proceeds normally
- Both systemic and tissue-specific DHT levels improve
- The androgenic signal is properly amplified
4. Testicular Health Preservation
Beyond testosterone, hCG maintains overall testicular function:
- Prevents testicular atrophy during TRT
- Preserves fertility potential
- Maintains other testicular-derived hormones (pregnenolone, DHEA)
- Supports the full steroidogenic pathway
This holistic testicular support creates conditions favorable for all downstream androgens including DHT.
5. Neurosteroid Pathway Support
The testicular steroidogenic pathway produces more than testosterone:
- Pregnenolone (the "mother hormone")
- DHEA and its metabolites
- Other neurosteroids
These compounds support brain health and may indirectly influence DHT-related neurological effects like confidence and motivation.
What Real People Are Saying
hCG is widely used in TRT protocols, and the community has extensive experience with its effects on androgenic function:
"Added hCG 250 IU 3x/week to my TRT and the difference was noticeable within a few weeks. Libido came back stronger, erections improved, and I generally felt more 'androgenic' if that makes sense. Labs showed my testosterone went up a bit, but the DHT increase was more significant. Clearly the hCG was supporting the conversion pathway." -- u/trt_optimization on r/Testosterone
"Was on TRT alone for years with okay results but always felt like something was missing. Added hCG and it was like the missing piece clicked into place. My DHT went from low-normal to solid mid-range. The subjective effects matched -- more drive, better in the gym, better in the bedroom." -- u/hcg_advocate on r/steroids
"Using hCG helped maintain my balls on TRT, which I expected. What I didn't expect was how much better I'd feel overall. My total T didn't change much since I was already injecting testosterone, but free T and DHT both came up. The intratesticular production must be contributing something the exogenous T doesn't provide." -- u/full_protocol on r/Peptides
These experiences reflect hCG use in TRT contexts under medical supervision.
Monitoring Your DHT Health with FixMyT
Understanding the relationship between testicular function and DHT requires comprehensive assessment. FixMyT provides this perspective.
The FixMyT symptoms quiz evaluates indicators across the androgen cascade:
- DHT-specific symptoms (libido quality, erectile function, confidence)
- Testosterone symptoms (energy, muscle, mood)
- Testicular function markers (size, fertility considerations)
- Upstream interference (estrogen, prolactin, cortisol)
The visual metabolic tree shows how DHT at Level 4 depends on testosterone production. If you are on TRT but still experiencing DHT-related symptoms, the issue may be insufficient testicular contribution. hCG can address this specific gap.
For those optimizing their TRT protocols, FixMyT helps identify whether testicular support is a priority target.
Research and Considerations
hCG has extensive clinical data supporting its effects on testosterone production and testicular function. The connection to DHT is mechanistically clear.
What the evidence supports:
- hCG directly stimulates Leydig cell testosterone production (well-established)
- Maintains intratesticular testosterone during TRT (demonstrated in studies)
- Preserves testicular volume and function (consistently shown)
- Testosterone is the obligate precursor for DHT (basic biochemistry)
- Generally well-tolerated with a decades-long safety record
What needs more research:
- Optimal hCG dosing specifically for DHT optimization
- Long-term effects on 5-AR activity and DHT:T ratios
- Individual variation in DHT response to hCG
- Comparison with other testicular support approaches
The evidence supports hCG for testosterone production; the DHT connection follows from testosterone's role as DHT precursor.
Disclaimer
This article is for educational and research purposes only. hCG is an FDA-approved prescription medication that requires medical supervision. Nothing in this article constitutes medical advice or a recommendation to use any substance.
hCG can increase estrogen through aromatization of the additional testosterone produced. Monitoring and management of estrogen may be necessary. If you are interested in hCG for TRT support or hormonal optimization, consult with a qualified healthcare provider.
Any decisions about health interventions remain your responsibility in consultation with appropriate medical professionals.
Learn More
- Full hCG Profile on PepGuide - Complete technical details and protocols
- Gonadorelin for GnRH Signaling - Alternative axis support
- FixMyT Metabolic Assessment - Understand your testosterone-DHT relationship
- Testosterone-HCG Article - More on hCG for testosterone support
References
-
Coviello AD, et al. "Low-dose human chorionic gonadotropin maintains intratesticular testosterone in normal men with testosterone-induced gonadotropin suppression." Journal of Clinical Endocrinology & Metabolism. 2005;90(5):2595-2602.
-
Lee JA, Ramasamy R. "Indications for the use of human chorionic gonadotropic hormone for the management of infertility in hypogonadal men." Translational Andrology and Urology. 2018;7(Suppl 3):S348-S352.
-
Kohn TP, et al. "The Effect of Subcutaneous Human Chorionic Gonadotropin on Testosterone Levels." Fertility and Sterility. 2019;111(4):e26.
-
Russell DW, Wilson JD. "Steroid 5 alpha-reductase: two genes/two enzymes." Annual Review of Biochemistry. 1994;63:25-61.
- Corona G, et al. "Testosterone supplementation and sexual function: a meta-analysis study." Journal of Sexual Medicine. 2014;11(6):1577-1592.